
Page 153 - 南京医科大学学报自然科学版
P. 153
第44卷第3期 张慧凤,肖旭东,龚佳康,等. 复发性抑郁障碍进展为谵妄性躁狂1例并文献复习[J].
2024年3月 南京医科大学学报(自然科学版),2024,44(3):440-444 ·443 ·
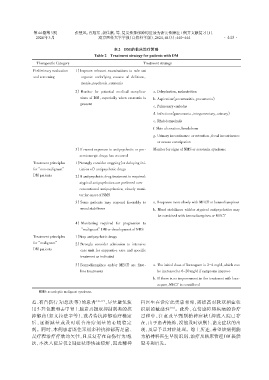
表2 DM的临床治疗策略
Table 2 Treatment strategy for patients with DM
Therapeutic Category Treatment strategy
Preliminary evaluation 1)Improve relevant examinations to rule out
and screening organic underlying causes of delirium,
mania,psychosis,catatonia
2)Monitor for potential medical complica⁃ a. Dehydration,malnutrition
tions of DM,especially when catatonia is b. Aspiration(pneumonitis,pneumonia)
present
c. Pulmonary embolus
d. Infections(pneumonia,integumentary,urinary)
e. Rhabdomyolysis
f. Skin ulceration,breakdown
g. Urinary incontinence or retention,fecal incontinence
or severe constipation
3)If recent exposure to antipsychotic or pro⁃ Monitor for signs of NMS or serotonin syndrome
serotonergic drugs has occurred
Treatment principles 1)Strongly consider stopping(or delaying ini⁃
for“non⁃malignant” tiation of)antipsychotic drugs
DM patients 2)If antipsychotic drug treatment is required:
atypical antipsychotics are preferred over
conventional antipsychotics; closely moni⁃
tor for onset of NMS
3)Some patients may respond favorably to a. Response more slowly with MECT or benzodiazepines
mood stabilizers b. Mood stabilizers with/or atypical antipsychotics may
be combined with benzodiazepines or MECT
4)Monitoring required for progression to
“malignant”DM or development of NMS
Treatment principles 1)Stop antipsychotic drugs
for“malignant”
2)Strongly consider admission to intensive
DM patients care unit for supportive care and specific
treatment as indicated
3)Benzodiazepines and/or MECT are first ⁃ a. The initial dose of lorazepam is 2-4 mg/d,which can
line treatments be increased to 6-20 mg/d if symptoms improve
b. If there is no improvement in the treatment with lora⁃
zepam,MECT is considered
MMS:neuroleptic malignant syndrome.
惹、有自伤行为/想法等)的患者 [16-17] ,尽量避免使 科医生在诊疗此类患者时,需提高对软双相症状
用 5⁃羟色胺和去甲肾上腺素再摄取抑制剂类的抗 识别的敏感性 [18] 。此外,在情感障碍疾病的诊疗
抑郁药(如文拉法辛等),或者待抗抑郁治疗稳定 过程中,注意及早甄别精神症状(抑或入院已存
后,逐渐减量或及时联合治疗剂量的心境稳定 在,由于患者掩饰,没能及时识别)、谵妄症状的出
剂。同时,本例患者既往采用多种抗抑郁药足量、 现,及早予以对症处理。综上所述,希望该病例能
足疗程治疗疗效均欠佳,且反复存在自伤行为/想 为精神科医生早期识别、治疗及临床管理 DM 提供
法,本次入院后仅 2 周症状即快速缓解,因此精神 思考和启发。