
Page 58 - 南京医科大学自然版
P. 58
第45卷第1期
· 52 · 南 京 医 科 大 学 学 报 2025年1月
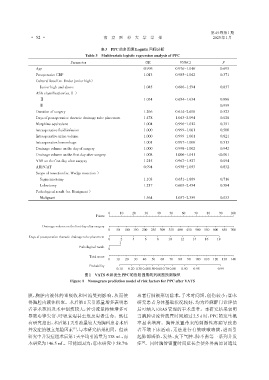
表3 PPC的多因素Logistic回归分析
Table 3 Multivariate logistic regression analysis of PPC
Parameter OR 95%CI P
Age 0.996 0.976-1.016 0.695
Preoperative CRP 1.013 0.985-1.042 0.371
Cultural level(vs. Under junior high)
Junior high and above 1.045 0.686-1.594 0.837
ASA classification(vs.Ⅰ )
Ⅱ 1.034 0.654-1.634 0.886
Ⅲ — — 0.999
Duration of surgery 1.266 0.614-2.608 0.523
Days of postoperative thoracic drainage tube placement 1.478 1.043-2.094 0.028
Morphine equivalent 1.004 0.996-1.012 0.351
Intraoperative fluid infusion 1.000 0.999-1.001 0.500
Intraoperative urine volume 1.000 0.999-1.001 0.821
Intraoperative hemorrhage 1.001 0.997-1.006 0.513
Drainage volume on the day of surgery 1.000 0.998-1.002 0.942
Drainage volume on the first day after surgery 1.008 1.006-1.011 <0.001
VAS on the first day after surgery 1.215 0.967-1.527 0.094
ARISCAT 0.994 0.938-1.053 0.832
Scope of resection(vs. Wedge resection )
Segmentectomy 1.103 0.651-1.869 0.716
Lobectomy 1.217 0.603-2.454 0.584
Pathological result(vs. Benignant )
Malignant 1.564 1.037-2.359 0.033
0 10 20 30 40 50 60 70 80 90 100
Points
Drainage volume on the first day after surgery
0 50 100 150 200 250 300 350 400 450 500 550 600 650 700
Days of postoperative thoracic drainage tube placement
0 2 4 6 8 10 12 14 16 18
1
Pathological result
0
Total score
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140
Probability
0.10 0.20 0.30 0.400.500.60 0.70 0.80 0.90 0.95 0.99
图1 VATS术后发生PPC的危险因素的列线图预测模型
Figure 1 Nomogram prediction model of risk factors for PPC after VATS
膜,胸腔内液体的重吸收和回流受到影响,从而使 患者行肺楔形切除术,手术时间短,创伤较小;②本
得胸腔内液体积聚。术后第1天引流量增多表明患 研究患者身体基础状况较好,均为经麻醉门诊评估
者手术范围及术中创伤较大,若引流量持续增多可 后可纳入ERAS管理的手术患者。本研究结果表明
导致心律失常、呼吸衰竭甚至危及患者生命。既往 当胸腔引流管放置时间超过2.5 d时,PPC的发生概
有研究指出,术后第1天引流量较大为胸科患者术后 率显著增高。胸管放置带来的刺激性疼痛导致患
并发症的独立危险因素 ,与本研究结果相同。但该 者不敢下床活动,无法进行有效咳嗽咳痰,进而引
[7]
研究中并发症组术后第1天平均引流量为338 mL,而 起肺部感染、发热、皮下气肿、肺不张等一系列并发
[8]
本研究为146.5 mL。可能原因为:①本研究中58.7% 症 。同时胸管留置时间延长会使外界病原菌通过