
Page 29 - 《南京医科大学学报》自然科学版2026年第2期
P. 29
第46卷第2期 张 强,褚 玥,马 高,等. CT平扫ASPECTS与CT灌注成像梗死核心体积不匹配的影响因素
2026年2月 分析[J]. 南京医科大学学报(自然科学版),2026,46(2):181-187 ·185 ·
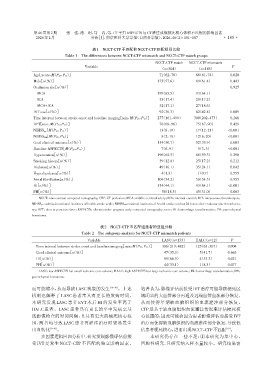
表1 NCCT⁃CTP不匹配和NCCT⁃CTP匹配组间比较
Table 1 The differences between NCCT⁃CTP mismatch and NCCT⁃CTP match groups
NCCT⁃CTP match NCCT⁃CTP mismatch
Variable P
(n=304) (n=145)
Age[years,M(P25,P75)] 71(62,78)0 68(61,74)0 0.020
Male[n(%)] 175(57.6)000 89(61.4)00 0.443
Occlusion site[n(%)] 0.925
MCA 199(65.5)000 93(64.1)00
ICA 53(17.4)00 25(17.2)00
MCA+ICA 52(17.1)00 27(18.6)00
IVT use[n(%)] 92(30.3)00 62(42.8)00 0.009
Time interval between stroke onset and baseline imaging[min,M(P25,P75)] 277(161,499) 300(202,473) 0.266
DPT[min,M(P25,P75)] 76(68,96)0 75(67,90)0 0.429
NIHSSpre [M(P25,P75)] 13(8,19)00 17(12,21)0 <0.001
NIHSS24h [M(P25,P75)] 8(2,18)0 12(6,20)00 <0.001
Good clinical outcome[n(%)] 154(50.7)000 52(35.9)00 0.003
Baseline ASPECTS[M(P25,P75)] 7(6,9)00 5(3,5)00 <0.001
Hypertension[n(%)] 196(64.5)000 86(59.3)00 0.290
Smoking history[n(%)] 39(12.8)00 25(17.2)00 0.212
Diabetes[n(%)] 49(16.1)00 35(24.1)00 0.042
Hyperlipidemia[n(%)] 4(1.3)00 1(0.7)00 0.555
Atrial fibrillation[n(%)] 104(34.2)000 50(34.5)00 0.955
HI[n(%)] 134(44.1)000 93(64.1)00 <0.001
PH[n(%)] 56(18.5) 45(31.0)00 0.003
NCCT:non⁃contrast computed tomography;CTP:CT perfusion;MCA:middle cerebral artery;ICA:internal carotid;IVT:intravenous thrombolysis;
NIHSSpre:admissionnational institutes of health stroke scale;NIHSS24h:national institutes of health stroke scaleat 24 hours after endovascular thrombecto⁃
my;DPT:door to puncture time;ASPECTS:alberta stroke program early computed tomography score;HI:hemorrhage transformation;PH:parenchymal
hematoma.
表2 NCCT⁃CTP不匹配组患者的亚组分析
Table 2 The subgroup analysis for NCCT⁃CTP mismatch patients
Variable LASC(n=133) HALC(n=12) P
Time interval between stroke onset and baseline imaging[min,M(P25,P75)] 306(219,482) 125(63,307) 0.004
Good clinical outcome[n(%)] 047(35.3) 005(41.7) 0.663
HI[n(%)] 089(66.9) 004(33.3) 0.021
PH[n(%)] 044(33.1) 001(8.3) 0.077
LASC:low ASPECTS but small ischemic core volume;HALC:high ASPECTS but large ischemic core volume;HI:hemorrhage transformation;PH:
parenchymal hematoma.
而可能缩小,从而导致LASC现象的发生 [19-20] 。上述 笔者认为,影像评估前接受IVT治疗可能导致梗死区
机制也解释了 LASC 患者常具有更长的发病时间。 域闭塞的大血管部分再通及远端血管血流部分恢复,
本研究发现 LASC 患者 EVT 术后 HI 的发生率高于 从而使得早期缺血脑组织的血流灌注部分恢复。
HALC 患者。LASC 患者具有更长的卒中发病至基 CTP是基于缺血脑组织血流灌注情况来评估梗死核
线影像检查的时间间隔,且具有更大的梗死核心范 心范围的,因此可能会因为患者影像评估前接受IVT
围,两者均导致 LASC 患者再灌注治疗时更易发生 治疗而使得缺血脑组织的血流灌注部分恢复,导致低
出血转化 [9-10] 。 估患者梗死核心,进而出现NCCT⁃CTP不匹配 。
[19]
多因素逻辑回归分析中,研究发现影像评估前接 本研究仍存在一些不足:①本研究为单中心、
受 IVT 是发生 NCCT⁃CTP 不匹配的独立影响因素。 回顾性研究,且研究纳入样本量较小。研究结果需