
Page 38 - 南京医科大学自然版
P. 38
第44卷第9期
·1210 · 南 京 医 科 大 学 学 报 2024年9月
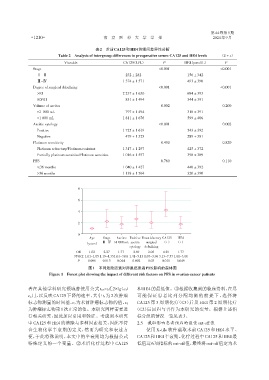
表2 术前CA125和HE4的组间差异性分析
Table 2 Analysis of intergroup differences in preoperative serum CA125 and HE4 levels (x ± s)
Viarable CA125(U/L) P HE4(pmol/L) P
Stage <0.001 <0.001
Ⅰ-Ⅱ 232 ± 282 0 156 ± 342
Ⅲ-Ⅳ 1 374 ± 1 571 493 ± 390
Degree of surgical debulking <0.001 <0.001
>R1 2 237 ± 1 630 684 ± 393
R0/R1 831 ± 1 494 344 ± 391
Volume of ascites <0.002 <0.200
≤1 000 mL 797 ± 1 494 318 ± 391
>1 000 mL 1 811 ± 1 676 599 ± 406
Ascitic cytology <0.001 <0.002
Positive 1 725 ± 1 619 543 ± 392
Negative 479 ± 1 325 289 ± 381
Platinum sensitivity <0.450 <0.820
Platinum refractory/Platinum resistant 1 317 ± 1 297 425 ± 372
Partially platinum sensitive/Platinum sensitive 1 016 ± 1 557 398 ± 389
PFS <0.760 <0.110
≤36 months 1 040 ± 1 427 440 ± 392
>36 months 1 138 ± 1 564 320 ± 390
8
6
4
2
0
Age Stage Ascites Pasitive Unsatisfactory CA125 HE4
(years) Ⅲ-Ⅳ >1 000 mL ascitic surgical (+) (+)
cytology debulking
OR 1.02 2.27 1.77 2.69 2.05 4.29 1.77
95%CI 1.01-1.05 1.19-4.351.01-3.08 1.41-5.13 1.07-3.96 3.13-7.57 1.01-3.08
P 0.006 0.013 0.044 0.002 0.03 0.011 0.049
图1 不同危险因素对卵巢癌患者PFS影响的森林图
Figure 1 Forest plot showing the impact of different risk factors on PFS in ovarian cancer patients
者在其他学科研究领域曾使用公式 t1/2=t1/[2×lg(c1/ 和HE4的最低值。③根据收集到的临床资料,在尽
c2)],以反映 CA125 下降的速率,其中 t1为 2 次肿瘤 可能保证患者比列分配均衡的前提下,选择将
CA125 第 3 周期化疗(C3)后及 HE4 第 2 周期化疗
标志物测量的时间差,c1为术前肿瘤标志物的值,c2
为肿瘤标志物第1次正常的值。本研究同样需要进 (C2)后回归与否作为本研究的变量。根据上述指
行相关研究,因此加以引用和验证。考虑到本研究 标分组的情况一览见表3。
中CA125和HE4的清除与多种因素相关,因此不符 2.5 截取影响患者预后的最佳cut⁃off值
合生物化学半衰期的定义,然而为研究和表述方 使用 X⁃tile 软件截取术前 CA125 和 HE4 水平、
便,于此特殊说明,本文中的半衰期均为根据公式 CA125和HE4半衰期、化疗过程中CA125和HE4最
特殊定义的一个变量。②术后化疗过程中 CA125 低值这6项指标的cut⁃off值,最终将cut⁃off值定为术